- Visibility 29 Views
- Downloads 6 Downloads
- DOI 10.18231/j.ijceo.2020.042
-
CrossMark

A study of serum homocysteine and serum vitamin B12 levels in patients with retinal vein occlusion and its correlation
Introduction
Retinal vein occlusions (RVOs) have been defined as retinal vascular disorders characterized by engorgement and dilatation of the retinal veins due to increased retinal venous blood pressure, with secondary intraretinal hemorrhages intraretinal & (and partially subretinal edema including foveal region and which can lead to hard retinal exudates due to deposits of lipids; and a varying degree of retinal ischemia leading to cotton wool spots as signs of it.[1], [2], [3], [4], [5], [6], [7], [8], [9]
RVOs are one of the most common causes of a retinal vascular abnormality and a frequent cause of visual loss.[10] Being recognized at least as early as 1855,[11] RVOs have been the subject of more than 3,000 publications so far.
Current estimates of the prevalence of RVOs are derived from major population-based studies, such as the Blue Mountains Eye Study, the Beaver Dam Eye Study, and a combined analysis of the Atherosclerosis Risk in Communities and Cardiovascular Health Studies.[12], [13], [14]
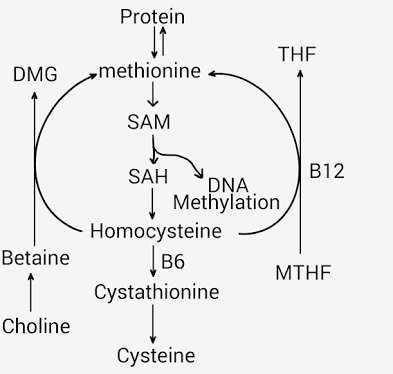
Homocysteine is an intermediary metabolite of essential dietary amino acid methionine, metabolised by remethylation to methionine or by trans-sulfuration to cysteine. Remethylation requires vitamin B12 (cobalamin) essentially.[15]
Hyperhomocysteinemia results from absence, mutation of any of these enzymes in these reactions. As depicted below, this can lead to deficiencies in folic acid, vitamin B6, or vitamin B12 cofactors can lead to elevated total plasma homocysteine (tHcy) levels.[16]
Hence, we will try to find correlation between Serum homocysteine and vitamin B-12 in patients with RVO. Additionally the study will elaborate serum homocysteine levels by means of ECLIA (Electro chemiluminescent immunoassay and vitamin B-12 levels by CMIA (chemiluminescent microparticle essay) and to find whether raised levels of homocysteine correlate with the types of RVO and also a correlation between low vitamin B12 levels and RVO and its types.
Materials and Methods
This study was conducted in out patient department (OPD) of Dr. D. Y. Patil medical college and hospital, Pimpri, Pune. A case control type of study was conducted from September 2017 to August 2019.
Sample size
100 (50 cases and 50 controls)
Inclusion criteria
Patients of all age groups coming in Ophthalmology OPD.
Patients coming with sudden loss of vision in Vitreo-retinal OPD.
Patients giving history of previous known attacks of RVO.
Exclusion criteria
Patients who have been diagnosed for HTN retinopathy.
Patients having other retinal pathologies resembling RVO like Eale’s disease, diabetic retinopathy, radiation retinopaty etc.
Patients having hazy/opaque media.
Methodology
Patients of all age group and any sex who are coming in vitreoretinal OPD of department of ophthalmology were studied.
Ethical clearance was obtained prior to study. Written informed consent was taken from all patients. 50 cases were selected as cases according to inclusion criteria. Age and sex matched controls were selected amongst non-diseased patients.
Data selection
Brief history was taken along with important demographic factors. Detailed history of other co-morbid conditions was taken.
Ocular examination including visual acuity (distant and near test types), BCVA (Best corrected visual acuity), intraocular pressure was measured by Goldmann applanation tonometer. Detailed slit lamp examination was done for anterior segment evaluation to find Neovascularization of iris (NVI), and Neovascularization of angle (NVA) etc were carried out.Dilated fundus of both eyes were evaluated. Types of RVO would be identified as central retinal vein occlusion (CRVO), branch retinal vein occlusion (BRVO), hemi-retinal vein occlusion (HCRVO) Retinal status was evaluated by direct ophthalmoscopy, slit lamp biomicroscopy by using 90D lens and indirect ophthalmoscopy after dilatation with Tropicamide/ Tropicamide plus eye drops. Serum Homocysteine was measured by Electro chemiluminescent immunoassay (ECLIA).
Hyperhomocysteinemia is defined as > 15 micromol/L
Serum Vitamin B-12 levels were assessed by Chemiluminescent Microparticle assay (CMIA) and levels would be assessed on following grades
<187 pg/ml – Low vitamin B12
187-883 pg/ml – Normal range
>883 pg/ml – High levels
Statistical analysis
Statistical analysis was done by using the soft ware Graphpad prism version 7. The results included mean values, standard deviations and p values calculated using unpaired students t test. Chi square was used where applicable.
Results
| Type of RVO | No of cases | Percentage |
| CRVO | 15 | 30% |
| BRVO | 30 | 60% |
| HCRVO | 4 | 8% |
| TVO | 1 | 2% |
In our study group, Highest number of cases were of BRVO (60%) and only one case of TVO (2%) was noted.
[Table 1] depicts BRVO being in the highest and TVO type being the least RVO type of cases.
| Homocysteine levels Micromol/L | RVO group | Control group |
| Mean | 23.80 | 12.43 |
| Std dev | 13.28 | 10.58 |
| P value | 7.7E-06 (P<0.0001) | |
| Inference | Homocysteine levels were significantly higher in RVO group when compared to control group |
[Table 2] shows us homocysteine levels in RVO and Control group. The average level of homocysteine in RVO and control group is found to be 23.80 and 12.43 whereas the standard deviation of homocysteine level in RVO group is 13.28 and control group is 10.58. Therefore we see that levels of homocysteine are significantly higher in RVO group in comparison with control group.
| Vitamin B-12 levels (pg/ml) | RVO group | Control group |
| Mean | 325.8 | 455.86 |
| Std dev. | 181.53 | 289.5 |
| P value | 0.00862 | |
| Inference | Vitamin B12 was significantly lower in case group compared to controls |
[Table 3] shows the Vitamin B-12 level in RVO and control group. The average value was found be 455.86 in control group and 325.8 in RVO group. The P value suggests that, Vitamin B12 was significantly lower in case group compared to controls
| RVO group | High HC level cases (>15micromol/L) | Normal HC level cases (4-15micromol/L) |
| Mean Vit-B 12 level (pg/ml) | 240.27 | 454.1 |
| Std dev | 108.09 | 195.64 |
| P value | 0.00013 | |
| Inference | Vitamin B-12 levels were significantly lower in cases with a higher Homocysteine level |
| Case+Controls | High HC level cases | Normal HC level cases |
| Mean Vit-B 12 level | 222.87 | 498.21 |
| Std dev | 100.56 | 256.79 |
| P value | 5.3E-11 (P<0.0001) | |
| Inference | Vitamin B-12 levels are significantly lesser in patients with a higher level of homocysteine irrespective of presence of RVO. |
[Table 5] show we observe Vitamin B-12 level is exceptionally higher in normal homocysteine level cases of both the groups, that is the RVO group and control group. The average value is found to be 498.21 in normal HC level and 222.87 in high HC level cases of control and RVO groups.
| HC levels | Mean | Std dev |
| CRVO | 24.27 | 16.58 |
| BRVO | 23.88 | 11.41 |
| P value | 0.93429 | |
| Inference | Non significant difference between mean HC levels in patients with CRVO vs. BRVO. |
[Table 6] compares HC levels specifically in patients of CRVO vs. BRVO. Non significant difference was found between mean HC levels in patients with CRVO vs. BRVO.
| Incidence of raised HC | Percentage | Incidence of low Vit B-12 | Percentage | |
| Cases | 30 | 60% | 14 | 28% |
| Controls | 9 | 18% | 10 | 20% |
The incidence of hyperhomocysteinemia was 60% in the cases with 28% incidence of low Vitamin B-12.
Discussion
It was found that the average age for males in RVO group was 56.98 and for the control group was 58.16 years. For RVO group the range of ages that were considered were 19-83 and for Control group 20-84 years. Martin SC et al.[17] measured the homocysteine levels in 70 patients with retinal vessel occlusion and compared them with homocysteine levels in 85 controls without any evidence of retinal vessel occlusion. The mean age of subjects was 66.2 years whereas it was 51.5 years for the patients with retinal vein occlusion.
The study was age and sex matched to avoid any bias arising due to age and gender of the patients. This was done by taking equal number of male and female control group as per age distribution in cases by randomization method. This is depicted in table 3 and corresponding figure. Bharathi Devi SR et al.[18] conducted a similar study where the patients were age and sex matched. Similarly many studies with age and sex matched of participants evaluating the homocysteine levels in patients of retinal vein occlusion were conducted.[19], [20], [21] Like in our study incidence of RVO increases with advancing age.
Study shows that the type of retinal vein occlusion. It was noted that Highest number of cases were of BRVO(60%) followed by CRVO(30%) and only one case of TVO was found. The prevalence rates of retinal vein occlusion per 1,000 persons were 4.42 for BRVO and 0.80 for CRVO, which were age- and gender-standardized to the 2008 population of the world aged 30 years and older.[16] Similarly in our study the prevalence of BRVO was higher when compared to other subtypes of RVO such as CRVO, HCRVO and TVO.
Study shows us homocysteine levels in RVO and Control group. The average level of homocysteine in RVO and control group is found to be 23.803 and 12.4274 whereas the standard deviation of homocysteine level in RVO group is 13.2805 and control group is 10.5811. Therefore we see that levels of homocysteine are significantly higher in RVO group in comparison with control group. Some authors hypothesized that elevated plasma homocysteine concentration could be a potential risk factor for RVO.[22], [23], [24] This was evident in our study. Minniti G et al.[19] correlated higher values of fasting homocysteine and low vitamin B-12 in patients with retinal vein occlusion. Mean plasma cysteine was significantly increased in patients with CRVO, suggesting that hyperhomocysteinemia may contribute to the pathogenesis of CRVO disorder was concluded in a study by Pinna A et al.[25] Martin SC et al[17] evaluated homocysteine levels in patients of retinal vein occlusion.
Chua B et al.[26] that elevated serum homocysteine levels in the blood is associated with the presence of RVO, independent of other risk factors.
Study depicts the Vitamin B-12 level in RVO and control group. [Normal levels of vitamin B-12 is defined as 187-883 pg/ml and for homocysteine it is > 15 micromol/L.] The average value was found to be 455.86ng/ml in control group and 325.8ng/ml in RVO group. The standard deviation in control group is significantly higher than RVO group. Minniti G et al. [19] concluded fasting homocysteine levels, low vitamin B12 levels, and hypertension are associated with a risk of RVO, especially for CRVO.
We can infer that average level of Vitamin B-12 in normal level of homocysteine participants was 454.1 ng/ ml and its standard deviation is 195.642 and in participants with high level of homocysteine it was 240.26 ng/ ml and its standard deviation is 108.08. These values depicts normal levels of vitamin B-12 in normal level of homocysteine and lower level in higher level of homocysteine.
Study depicts Vitamin B 12 levels in context of Homocysteine levels irrespective of Case/control group. We observed that Vitamin B-12 level is normal in homocysteine level cases of both the groups, that is the RVO group and control group. The average value is found to be 498.213 in normal HC level and 222.872 in high HC level cases of control and RVO groups. We need to consider the patients with higher homocysteine and lower vitamin B-12 in context of a risk factor for development of RVO as this is an independent risk factor in control group patients. [22], [26]
HC levels specifically in patients of CRVO vs. BRVO. Non significant difference was found between mean HC levels in patients with CRVO vs. BRVO. The mean in CRVO group was 24.274 micromol/L and 23.8767 micromol/L in BRVO group. However, both are raised considering the cut off for normal range of 4-15 micromol/L. [26]
Study highlights the incidence of increased HC and low Vit B-12 in cases vs. controls. The incidence of hyperhomocysteinemia was 60% in the cases with 28% incidence of low Vitamin B-12 whereas in controls incidence of hyperhomocysteinemia was 18% with 20% incidence of low Vitamin B-12
Conclusion
Homocysteine levels were found to be significantly elevated in patients having retinal vein occlusion when compared to controls.
Vitamin B-12 levels were significantly lesser in patients of retinal vein occlusion when compared to controls.
All the patients having hyperhomocysteinemia have significantly lower levels of vitamin B12.
Patients having no underlying systemic conditions, Serum Homocysteine is the prime factor to study in patients with Retinal vein occlusion.
All patients with RVO should mandatorily be evaluated for presence of low B-12 levels and hyperhomocysteinemia.
Source of Funding
None.
Conflict of Interest
None.
References
- S S Hayreh. Occlusion of the central retinal vessels.. Br J Ophthalmol 1965. [Google Scholar]
- S S Hayreh. An experimental study of the central retinal vein occlusion. Trans Ophthalmol Soc UK 1964. [Google Scholar]
- G Coscas, P Dhermy. . Occlusions veineusesrétiniennes 1978. [Google Scholar]
- Sohan Singh Hayreh. Classification of central retinal vein occlusion. Ophthalmol 1983. [Google Scholar]
- . Baseline and early natural history report. Arch Ophthalmol 1993. [Google Scholar]
- . Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmol 1995. [Google Scholar]
- . The central vein occlusion study group n report. A randomized clinical trial of early panretinal photocoagulation for ischemic central vein occlusion. Ophthalmol 1995. [Google Scholar]
- Sohan Singh Hayreh, Marie R. Klugman, Meena Beri, Alan E. Kimura, Patricia Podhajsky. Differentiation of ischemic from non-ischemic central retinal vein occlusion during the early acute phase. Graefes Arch Clin Exp Ophthalmol 1990. [Google Scholar]
- Gabriel Coscas, Alain Gaudric. Natural course of nonaphakic cystoid macular edema. Surv Ophthalmol 1984. [Google Scholar]
- R P Maurya. More about retinal vein occlusion. Ind J Clin Exp Ophth 2017. [Google Scholar]
- R Liebreich. Ueber die Farbe des Augenhintergrundes. Albrecht Von Graefes Arch Ophthalmol 1855. [Google Scholar]
- R Klein, B E Klein, S E Moss, S M Meuer. The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc 2000. [Google Scholar]
- P Mitchell, W Smith, A Chang. Prevalence and associations of retinal vein occlusion in Australia. The blue mountains eye study. Arch Ophthalmol 1996. [Google Scholar]
- T Wong, E Larsen, R Klein, P Mitchell, D Couper, B Klein. Cardiovascular risk factors for retinal vein occlusion and arteriolar emboli: the atherosclerosis risk in communities & cardiovascular health studies. Ophthalmol 2005. [Google Scholar]
- Weiwei Liu, Liang Xu, Jost B. Jonas. Vein occlusion in Chinese subjects. Ophthalmol 2007. [Google Scholar]
- J Q Zhou, L Xu, S Wang, Y X Wang, Q S You, Y Tu. The 10-year incidence and risk factors of retinal vein occlusion: the Beijing Eye Study. Ophthalmol 2013. [Google Scholar]
- Steven C Martin, S Rauz, J E Marr, N Martin, A F Jones, P M Dodson. Plasma total homocysteine and retinal vascular disease. Eye 2000. [Google Scholar]
- Subramaniam Rajesh Bharathi Devi, Ganesan Suganeswari, Tarun Sharma, Maruthamuthu Thennarasu, Narayanasamy Angayarkanni. Homocysteine induces oxidative stress in young adult central retinal vein occlusion. Br J Ophthalmol 2012. [Google Scholar]
- Giuseppe Minniti, Maria Grazia Calevo, Alessandro Giannattasio, Paola Camicione, Ugo Armani, Renata Lorini. Plasma Homocysteine in Patients with Retinal Vein Occlusion. Eur J Ophthalmol 2014. [Google Scholar]
- Sasan Moghimi, Zahra Najmi, Hooshang Faghihi, Reza Karkhaneh, Mohammad Sadegh Farahvash, Maryam Maghsoudipour. Hyperhomocysteinemia and central retinal vein occlusion in Iranian population. Int Ophthalmol 2008. [Google Scholar]
- Rajiv Khandekar, Gigani Salim, Mohammed Al Ali, Salman Ramzi, Fahad Al Wadani. Hyperhomocysteinia is a risk factor for retinal venous occlusion: A case control study. Indian J Ophthalmol 2014. [Google Scholar]
- Bruce A Brown, Jeffrey L Marx, Thomas P Ward, Rodney D Hollifield, John S Dick, John J Brozetti. Homocysteine: a risk factor for retinal venous occlusive disease. Ophthalmol 2002. [Google Scholar]
- Gianluca Sottilotta, Vincenzo Oriana, Caterina Latella, Francesca Luise, Angela Piromalli, Francesca Ramirez. Role of hyperhomocystinemia in retinal vascular occlusive disease. Clin Appl Thromb Hemost 2007. [Google Scholar]
- Brian Chua, Annette Kifley, Tien Y. Wong, Paul Mitchell. Homocysteine and retinal emboli: the blue mountains eye study. Am J Ophthalmol 2006. [Google Scholar]
- Antonio Pinna, Ciriaco Carru, Angelo Zinellu, Stefano Dore, Luca Deiana, Francesco Carta. Plasma homocysteine and cysteine levels in retinal vein occlusion. Invest Ophthalmol Vis Sci 2006. [Google Scholar]
- Brian Chua, Annette Kifley, Tien Y. Wong, Paul Mitchell. Homocysteine and retinal vein occlusion: A Population-based study. Am J Ophthalmol 2005. [Google Scholar]