
Introduction
Congenital lid eversion is a rare clinical event which was first reported by Adams in 1896 who used the term ‘double congenital ectropion’. It has a predilection for the superior conjunctival fornix. In this condition, the eyelid is completely turned out, with prolapsed conjunctiva and chemosis. Majority of the cases have bilateral presentation. The exact etiology remains unknown. However, local or systemic causes leading to anterior lamellar shortening or posterior lamellar elongation or prolapse can predispose to eversion of the eyelid. The treatment depends on the timing and severity of presentation. Early presentations usually respond well to conservative management. Surgical management is reserved for cases with late presentations or with complications or cases not responding to medical management. Herein, we present two cases of neonates with congenital total eversion of upper eyelid and conjunctival prolapse, which were effectively treated with conservative management.
Case 1
A 2-days old male baby presented to us with total eversion of right upper eyelid since birth. The baby was born at full term by normal vaginal delivery to a 30-year-old primigravida. Perinatal course was uneventful. On examination, there was marked conjunctival chemosis of right upper eyelid, associated with conjunctival ulceration and oozing of blood (Figure 1). No abnormality was detected on systemic examination by the paediatrician.
The child was treated conservatively with frequent lubricants (carboxymethylcellulose 1%), antibiotic eye ointment and 5% hypertonic saline patching over the chemosed conjunctiva. At one week follow up, the chemosis resolved markedly and conjunctiva was manually reposited after instillation of topical anaesthetic drops. The eyelid was taped with adhesive tapes. At ten days follow up, chemosis was resolved completely and baby was able to open the eyelid spontaneously.
Case 2
A 1-week-old male baby presented with total eversion of right upper eyelid associated with severe conjunctival chemosis. The left upper eyelid ectropion was present without any conjunctival prolapse (Figure 2). The baby was born full term by normal vaginal delivery. Perinatal course was uneventful. On examination, the patient had lamellar ichthyosis with scaly skin around the periorbital and perioral region. There was complete eversion of the right upper eyelid with conjunctival prolapse and marked chemosis. The left upper eyelid also had ectropion without any conjunctival chemosis. On retracting the chemosed conjunctiva, the cornea and globe were found to be normal.
Conjunctival repositioning was attempted but was unsuccessful due to anterior lamellar shortening. Conservative management with frequent lubricants, antibiotic ointment and hypertonic saline patch was given for 1 week. Dermatologist advice was followed for the treatment of lamellar ichthyosis by applying skin moisturizers. At 2 weeks follow up, the condition improved significantly with resolution of conjunctival chemosis in the right eye and improvement of ectropion in both eyes.
Table 1
Cases of congenital upper eyelid eversion successfully treated with conservative management
|
S No. |
Authors |
Age/Sex |
Laterality |
Conjunctival chemosis |
Management |
Outcome |
|
1. |
Watts and Dapling1 |
Newborn/M |
Unilateral |
++ |
Conservative |
Resolution in 1 week |
|
2. |
Maheshwari2 |
5d/M |
Bilateral |
+++ |
Conservative |
Resolution in 4 weeks |
|
3. |
Awoyesuku et al3 |
8h/M |
Bilateral |
+++ |
Conservative |
Resolution in 4 weeks |
|
4. |
Cingu et al.4 |
3h/M |
Bilateral |
++ |
Conservative |
Resolution in 3 days |
|
5. |
Chhabra et al.5 |
6h/M |
Bilateral |
++ |
Conservative |
Resolution in 4 weeks |
|
6. |
Ibraheem6 |
6d/F |
Bilateral |
+++ |
Conservative |
Resolution in 5 days |
|
7. |
Dohvoma et al.7 |
6h/M |
Bilateral |
+++ |
Conservative |
Resolution in 3 weeks |
|
8. |
Kirkpatrick et al.8 |
40 week /F |
Bilateral |
++ |
Conservative |
Resolution on day 26 |
|
9. |
Dzidzinyo et al.9 |
Newborn/F |
Bilateral |
+++ |
Conservative |
Resolution in 2 days |
|
Newborn/M |
Bilateral |
++ |
Conservative |
Resolution in 4 days |
||
|
Newborn/M |
Bilateral |
++ |
Conservative |
Resolution in 5 days |
||
|
10. |
Güdeloğlu10 |
2h/M |
Bilateral |
+++ |
Conservative |
Resolution in 3 weeks |
|
11. |
Our case |
2d/M |
Unilateral |
+++ |
Conservative |
Resolution in 10 days |
|
7 d/M |
Bilateral |
+++ |
Conservative |
Resolution in 2 weeks |
Figure 1
a: Clinical photograph of a 2 days old baby with right upper eyelid total eversion and marked conjunctival chemosis associated with oozing of blood from areas of conjunctival ulcerations. b: Clinical photograph of the same baby at 10 days follow up post conservative management, showing resolution of conjunctival prolapse
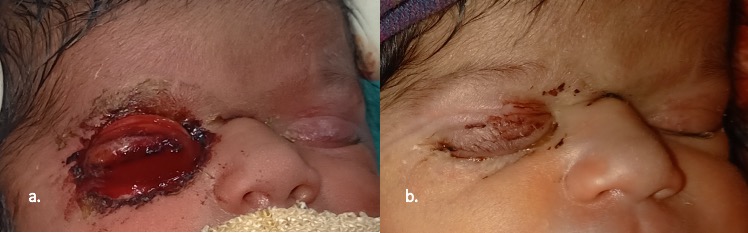
Figure 2
a: Clinical photograph of a 7 days old baby with lamellar ichthyosis, showing complete eversion of the right upper eyelid with markedly chemosed conjunctiva. Upper lid ectropion is also present in the left eye. b: On retraction of the upper eyelids, normal cornea is seen. 2c. Clinical photograph of the baby at 2 weeks follow up after medical management and eyelid taping, showing complete resolution of the ectropion in both the eyes

Discussion and Review of Literature
Congenital total eversion of upper eyelid is an uncommon entity of unknown etiology. Several possible mechanisms have been proposed. Orbicularis hypotonia, birth trauma, vertical shortening of the anterior lamella or vertical elongation of the posterior lamella of the eyelid, failure of the orbital septum to fuse with the levator aponeurosis, absence of effective lateral canthal ligament and lateral elongation of the eyelid have all been proposed as possible mechanisms responsible for the eversion. Venous stasis during delivery may cause marked chemosis and prolapse of the conjunctiva, causing eversion of the eyelids. Once everted orbicularis spasm may act as sphincter, that leads to a vicious cycle of conjunctival strangulation and edema, secondary to venous stasis. The chemosed conjunctiva protects the cornea from exposure and hence, corneal complications are rare. However, a case of corneal perforation has been reported in a baby with Down syndrome11 Adeoti et al. reported that one of the three cases had manifestations of neonatal sepsis.12
The condition is typically bilateral, but unilateral cases have also been described. One of our case had unilateral presentation, the other had bilateral asymmetric presentation. Higher incidence is seen in black infants, trisomy 21, infants born with collodion skin disease and children of multiparous mothers.13 It has also been associated with prolonged and difficult labor. Both of our cases were born to primigravida with uneventful labor. One of our cases had associated lamellar ichthyosis leading to anterior lamellar shortening and eversion of upper eyelid.
Several management modalities both conservative and surgical have been proposed for management of congenital eyelid eversion. The goal of management is to prevent desiccation of the exposed conjunctiva and allow spontaneous inversion of the lid. Conservative treatment involves the use of ointments and lubricants, topical prophylactic antibiotics and patching with 5% hypertonic saline. The mechanism by which the 5% hypertonic saline soaked gauze dressing worked was put forward by Voet et al.14 He suggested that osmosis of fluid from edematous tissues through the semi permeable subconjunctival membrane, is encouraged by the hypertonicity of the patch. This leads to the resolution of the edema and subsequent lid reversion. Review of literature revealed conservative management is an effective way of treating this condition by several authors (Table 1).
Surgical management should only be reserved for cases and patients presenting late to prevent keratinisation of conjunctiva and amblyopia. Surgical treatment includes scarification of the exposed conjunctiva, temporary tarsorrhaphy, subconjunctival injection of hyaluronic acid, fornix sutures, full thickness skin graft to the upper lid, and compression eyelid sutures.
We managed both of our cases by topical lubricants, antibiotics and hypertonic saline initially, which was then followed by conjunctival repositioning and taping of the eyelids. These cases illustrate that early repositioning of the conjunctiva is needed to break the cycle leading to conjunctival ulceration, progressive eyelid edema, conjunctival chemosis and further eversion. If not treated early, it could lead to complications like secondary infections and keratinization of the conjunctiva.
Conclusion
We demonstrate with our two cases that the congenital total eversion of the upper eyelids is a rare condition with an alarming presentation for the parents as well as the healthcare professionals. However, timely and appropriate management can prevent complications. We aim to create awareness amongst ophthalmologists and oculoplastic surgeons for this entity and advocate that successful outcomes can be achieved by conservative management.