
Introduction
Age-related macular degeneration (ARMD), the third common cause of visual impairment results for 8.7% of the total blindness globally. In industrialized countries, ARMD is becoming one of the primary causes of visual impairment.1 The number of people with ARMD is predicted to increase from three to six million by the year 2020. This is due to a decrease in avoidable blindness, due to anterior segment pathologies and the increasing life expectancy of the global population. World Health Organization has included ARMD in it’s action plan, to address avoidable blindness in VISION 2020 program.2
The prevalence of ARMD varies from 1.2% to 29.3%.3 From various studies, it is well established that ARMD is frequent in coloured races and the prevalence varies from 1.1% in South India4 to 17.4% in Africa.5 The prevalence rate was found to be 4.7% in a study done in North India.6
Body mass index has been related to incidence of visually significant ARMD in men. Waist to hip ratio as compared to BMI is more significantly associated with risk of developing ARMD in females.7 High prevalence of ARMD was also associated with the present and past history of systemic diseases like cardiovascular disease, hypertension, arteriosclerosis and lung infection.8 Amongst modifiable risk factors, diet and smoking are important risk factors for ARMD. Smoking is one of the most consistently documented modifiable risk factor in majority of workers. In a recent study, from New Zealand strong history of smoking was present in 26.8% of all ARMD cases. History of smoking was the most important preventable cause of ARMD as seen in pooled data from Europe, America and Australia. The damage could be directly through oxidative stress, indirectly by promotion of atherosclerosis or by decreasing macular pigment density. The duration of smoking and not amount of smoking was found to be associated with ARMD.9
With this background, this study was aimed to evaluate prevalence of age related macular degeneration in elderly population over 50 years of age and to determine its risk factors.
Materials and Methods
This was a analytical cross sectional study conducted in the department of ophthalmology in a Tertiary Hospital and research centre in Western Maharashtra from October-2017 to August- 2019. Patients of age related macular degeneration > 50 years who attended the outpatient department (OPD) for treatment. Sample size of 300 was taken by using Epi 7 Info software, taking confidence interval of 95%, prevalence of 5% and error of 2.5%. Study was performed after getting clearance from Institute Ethical Committee. Patients having corneal, lenticular or vitreous opacity in which fundus examination was not possible were excluded from study. Conditions such as polypoidal, choroidalvasculopathy, retinal angiomatous proliferation, myopic chorioretinal degeneration, any macular dystrophies were also excluded. Written, informed consent was obtained from all patients.
Data pertaining to socio-demographic factors, personal medical history and lifestyle factors such as smoking was collected by interview technique and documented in predesigned data collection tool. Patients were categorised as smokers and non smokers based on duration of smoking. If duration of smoking was less than one year they were categorised as non smokers.
B.M.I. was calculated as the individual’s weight in kilograms divided by the square of the individual’s height in meters. Obesity was defined as BMI>30kg/m2.
Patients were evaluated for the following-
Uncorrected visual acuity, best corrected visual acuity and pinhole improvement of vision was checked.
Slit-lamp bio-microscopy, was done to evaluate for corneal opacity, optically clear anterior chamber, status of lens and also checked for any opacities in the vitreous.
Fundus was examined with Direct, Indirect Ophthalmoscope and slit lamp biomicroscopy using 90 D lens through a dilated pupil with tropicamide (0.8%) and phenylephrine (5%).
Specific signs of ARMD were looked for and were graded into following 4 groups based on examination findings.
Table 1
AREDS classification of ARMD
Patients having changes of ARMD were then examined using Amsler’s grid Figure 1, which is most commonly used and comprises of high contrast white grid on a black background.
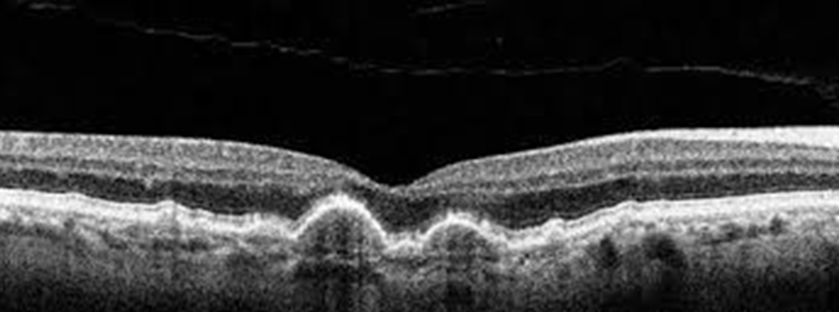
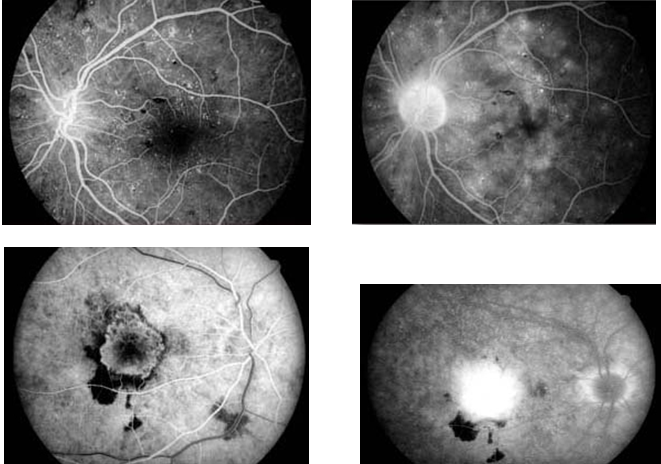
Optical coherence tomography and FFA was done for confirmation of clinical findings in every patient.
Statistical analysis data management and analysis was done using Microsoft excel and Epi-info software. The frequency distribution and graph was prepared for the variables. The categorical variables were assessed using Pearson chi-square test. All the tests were considered significant if p value comes to be less than 0.05.
Results
We studied 300 patients attending ophthalmology OPD of a tertiary care hospital in Western Maharashtra. Risk factors such as age, sex, residence, history of smoking, BMI and family history of ARMD were studied in patients with ARMD. Diagnosis of ARMD was made on dilated fundus examination and was confirmed on FFA and OCT.
Table 2 shows prevalence of ARMD. Out of 300 individuals studied, it was observed that in our study, 24 (8.0%) had ARMD.
Table 3
Distribution of patients according to age
Table 3 shows distribution of patients according to age group. It was observed that among 24 patients having ARMD, 3 (12.5%) patients were between 51-60 years, 5 (20.8%) patients were between 61-70 years, 10 (41.7%) patients were between 71-80 years and 6 (25.0%) patients were between 81-90 years. There was statistically significant association between increasing age and ARMD positivity with p value less than 0.05.
Table 4
Distribution of patients according to Sex
| Sex | ARMD | Total (%) | |
| Present (%) | Absent (%) | ||
| Male | 4 (16.7) | 144 (52.2) | 148 (49.3) |
| Female | 20 (83.3) | 132 (47.8) | 152 (50.7) |
| Total | 24 (100.0) | 276 (100.0) | 300 (100.0) |
Table 4 shows distribution of patients according to sex. It was observed that among 24 patients with ARMD, 4 (16.7%) were males and 20 (83.3%) were females while among individuals without ARMD, 144 (52.2%) were males and 132 (47.8%) were females. There was statistically significant association between female sex and ARMD positivity with p value less than 0.001.
Table 5
Distribution of patients according to BMI
| BMI | ARMD | Total (%) | |
| Present (%) | Absent (%) | ||
| 18.5 – 24.9 | 6 (25.0) | 88 (31.9) | 94 (31.3) |
| 25.0 -29.9 | 18 (75.0) | 164 (59.4) | 182 (60.7) |
| 30.0- 34.9 | 0 | 24 (8.7) | 24 (8.0) |
| Total | 24 (100.0) | 276 (100.0) | 300 (100.0) |
Table 5 shows distribution of patients according to BMI. It was observed that among 24 patients with ARMD, 6 (25.0%) were having BMI between 18.5 – 24.9, 18 (75.0%) were between 25.0 – 29.9 while among individuals without ARMD, 88 (31.9%) were between 18.5 – 24.9, 164 (59.4%) were between 25.0 – 29.9 and 24 (8.7%) were between 30.0 – 34.9. There was no statistically significant association found between BMI and ARMD with p value more than 0.05.
Table 6
Distribution of patients according to history of Smoking
| Smoking | ARMD | Total (%) | |
| Present (%) | Absent (%) | ||
| Smokers | 4 (16.7) | 69 (25.0) | 73 (24.3) |
| Non-smokers | 20 (83.3) | 207 (75.0) | 227 (75.7) |
| Total | 24 (100.0) | 276 (100.0) | 300 (100.0) |
Table 6 shows distribution of smokers in the group studied. It was observed that among patients with ARMD, 4 (16.7%) were smokers and 20 (83.3%) were non-smokers while among individuals without ARMD, 69 (25.0%) were smokers and 207 (75.0%) were non-smokers. There was no statistically significant association found between smoking and ARMD in our study with p value more than 0.05. Association between number of cigarettes smoked with the risk of developing ARMD was not studied.
Table 7
Distribution of patients according to family history of ARMD
| Family history of ARMD | ARMD | Total (%) | |
| Present (%) | Absent (%) | ||
| Present | 13 (54.2) | 22 (8.0) | 35 (11.0) |
| Absent | 11 (45.8) | 254 (92.0) | 265 (89.0) |
| Total | 24 (100.0) | 276 (100.0) | 300 (100.0) |
Table 7 shows distribution of patients according to family history of ARMD. It was observed that among patients with ARMD, 13 (54.2%) were having positive family history of ARMD and 11 (45.8%) were having no family history of ARMD while among individuals without ARMD, 22 (8.0%) were having positive family history of ARMD and 254 (92.0%) were having no family history of ARMD. There was statistically significant association between family history of ARMD and ARMD positivity with p value less than 0.001.
Discussion
India is the second most populous country in the world, with over 1.18 billion people (estimate for April, 2010), more than a sixth of the world's population. With 17.3% of the world's population already, India is projected to be the world's most populous country by 2025. By 2050, it is estimated that its population will exceed 1.6 billion people.10 With rapidly increasing aging population in India (life expectancy at birth males /females: 67/70 in year 2016)11 and with blindness due to cataract being addressed more vigorously (cataract surgery rate of 4,500 / million population in 2005), the age-related blinding causes of posterior segment will be more important in the coming years.12
We studied 300 individuals reporting to the Eye OPD of a tertiary care hospital in Western Maharashtra. 24 individuals were found to have ARMD for a prevalence of ARMD of 8.0%. The prevalence of ARMD in different studies varies from 1.2% to 29.3%.3, 13 According to previous three significant reports by Aravind Comprehensive Eye Study,14 Andhra Pradesh Eye Study15 and India Eye Study,16 prevalence of ARMD ranges between 1.4 to 1.8 percent within India. Also prevalence worldwide varies between 1.51% as was found in Beaver Dam Eye Study17 and 1.81% found in Blue Mountain Eye Study.18 Another study done in Northern India showed prevalence of 20.5%.19 This wide range of prevalence of ARMD may be due to different sampling methods, diagnostic criteria and associated risk factors varying with different geographic areas.
In our study, we found that as age advances, chances of developing ARMD increase. In the age group of 51-60 years, there were 3 patients (12.5%), in 61-70 years age group, there were 5 patients (20.8%), 10 patients (41.7%) in 71-80 years age group, and in 81-90 years age group, there were 6 patients (25.0%). We found that ARMD was more in the 71-80 years age group. As age advances, chances of developing ARMD increase. Similar results have been found in various studies. In a study done in Maharashtra by Singare et al., increasing age was found to be a risk factor which was 11.15% above 70 years of age.20 According to National Eye Institute (NEI), Maryland, USA, the prevalence of AMD was 2.1% in age group 40-49 years, whereas, it increased significantly to 35% in the subjects over 80 years of age.21 A study was done by Nirmalan et al. in Aravind Eye Hospital to study the prevalence of vitreoretinal disorders in a rural population of Southern India in the year 2004. The results of the study showed that the prevalence of early and late ARMD increased with increasing age (p value <0.001).14 Also this association between age and ARMD is consistent with various other studies in different parts of world.18, 22
In our study, we found that females were at higher risk of developing ARMD. We found that there were 83.3% females as compared to 16.7% males in our study. A study done by Pokharel et al. in Nepal found that the prevalence of ARMD in females was higher with female preponderance in ratio of 2.5:1.23 The cause may be greater longevity among females. In Blue Mountain eye study, females had a higher risk of developing ARMD.24 In some studies, males were found to have a higher prevalence of ARMD due to smoking habits. A study done by Miho Yasuda et al. showed that males had higher risk of developing ARMD.25 However in some studies, there was no difference found in prevalence of ARMD between males and females.26
Our study showed no significant association between BMI and ARMD. Jaisankar et al., at Sankara Netralaya studied correlation of various obesity indices with dry ARMD. They also found no significant association between obesity and dry ARMD.27 Studies done in different parts of world also showed no association between ARMD and obesity.28, 29 A study done by Zhang et al. in China showed linear correlation between BMI and risk of developing ARMD.30 Increasing body weight causes several physical changes, including a higher level of oxidative stress, a higher risk of inflammatory processes and imbalance of lipids, which is involved in ARMD pathogenic mechanisms.31 The migration and infiltration of monocyte could be regulated by these pro-inflammatory factors, causing a disturbance in the function of the RPE which might lead to ARMD.
Smoking was not found to be a significant risk factor in our study. We found that 16.7% of patients with ARMD were smokers, where as 83.3% were non smokers. A study done by Sucheta et al. at H.V Desai Hospital also found no significant association between smoking and ARMD.32 This may be due to variation in smoking habits and the greater number of females in our study. The French POLA study (Pathologies Ocularies Liees a l'Age) found that both current and former smokers had the highest risk for developing macular degeneration.33 A study done by Krishnaiah et al. found that smoking was not found as a statistically significant risk factor in occurrence of ARMD.14 Cigarette smoking is the only risk factor other than age that has been consistently identified in many large studies. The mechanism of action by which smoking could affect the retina, RPE or choroid is not known yet. However, the hypothesis is that ARMD is the result of cumulative oxidative insults to the outer retina. Smoking is known to lower levels of circulating antioxidants.
Family history of ARMD was a significant risk factor found in our study. In our study, 54.2% had a positive family history of ARMD. Family history was found to be significant in many studies. A study was done by Usha Chakravarti et al. to identify various risk factors of ARMD. In their study, they found family history to be a significant risk factor. There are various genes implicated in pathogenesis of ARMD such as complement factor H and C3, LOCS 3877, HTRA 1. 34 A recent study done by Cecile Delcourt et al also showed that family history was associated with an increased risk of early and late ARMD.(OR=1.25 and OR=1.89, respectively; P<0.0001).35
Conclusion
The prevalence of ARMD in our study was 8%, with age group of 71-80 years most commonly affected. Females were found to have higher prevalence of ARMD in our study. Smoking and obesity, history of cardiovascular disease, cataract surgery and sunlight exposure were not found to have a significant association with the risk of developing ARMD in our study. Family history of ARMD was a significant risk factor found in our study. Many such studies need to be done in future to establish more risk factors associated with development of ARMD.